



There is a lot of information out there about Janda’s “Lower Cross Syndrome” – It is characterised by anterior hip tilt and an increased lumbar lordosis. According to what you read, this may – or indeed, may not lead to lower back pain or other musculoskeletal problems.
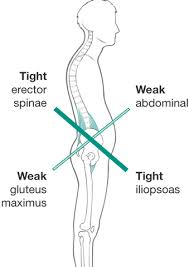 The fact that this syndrome led to pain was a fairly well accepted theory for many years and a lot of physiotherapy was focused on remedying this anterior hip tilt through the stretching of “tight” hip flexors and strengthening of the “weak” or “loose” core and somewhat amnesiac glutes. (How, exactly do glutes forget to fire? That is something to address at another point).
The fact that this syndrome led to pain was a fairly well accepted theory for many years and a lot of physiotherapy was focused on remedying this anterior hip tilt through the stretching of “tight” hip flexors and strengthening of the “weak” or “loose” core and somewhat amnesiac glutes. (How, exactly do glutes forget to fire? That is something to address at another point).
Recently, online guru against guru’s – Greg Lehman has shone doubt upon the whole biomechanical premise of Lower Cross Syndrome causing pain and has set out some pretty decent analysis of recent studies. Indeed, the data would seem to suggest that there is little correlation or causation between such a “syndrome” and any type of pain at all.
In terms of personal experience or case studies of n=1 vs scientific rigour, there isn’t really much of a fight. Scientific rigour should win out every single time. The multiple of “Clinical Experience” is not, and never will be, “Randomised Control Trial”, and as such, I certainly don’t wish to state that my experience has the scientific validity of Greg’s approach.
That being said, I am trying to make sense of an injury that I sustained some 8 weeks ago, and as such, this is how it has gone so far.
The Situation
I’m a fell runner and a long distance running affectionado. I have strong hip flexors and a weak “core” (for want of a better word to describe the wobbly bit between my hips and my shoulders), a classic “Thomas” test reveals “shortened” hip flexors with a significant anterior hip tilt, and has done for, oooh, the last 6 years.
So far, so “long distance runner” and so far, a fair amount of apparently objective signs that a number of MSK therapists might look at, purse their lips, shake their heads and say “oooh, we’re going to have to do something with you”, thinking about technical things to do with the hips and sacrum (like upslips and nutations).
The Problem
Started a year ago in August 2016. In the last 200m of a race (only about 10km long), I sprinted at flat out pace down a hill, legs at full stretch – with the back leg pulling me into lumbar lordosis as the front leg stretched out at the extremes of stride. The upshot of this was that I developed constant and consistent pain in my right hip flexor/adductor over the next few days.
 It was aggravated by running, so I took a few weeks off, but still did a bit of hill walking.
It was aggravated by running, so I took a few weeks off, but still did a bit of hill walking.
By 6 weeks down the line, rest had not healed it, I started tentatively running again and added in weight training and hip rehab, going along the lines of “well… if rest isn’t helping, then I should start thinking about getting it moving again”. Throughout winter I continued with this with the pain slowly getting less, but never actually going away.
Fast Forward to April/May/June
I was gradually increasing my weekly distance and ascent in preparation for August and the TDS- a 110km 7000m race in the alps. I was being sensible and increasing slowly, getting up to 80km and 4000m ascent per week.
By this time I still had not totally got rid of the adductor pain, but it was affecting me less and less. However, the weakness in my “core” and excessive strength in my hip flexors may have been putting strain on my hip flexor complex and lumbar and sacro-iliac area. Then again – it might not.
Early June, I was having a good week, but on the Friday I felt a little soreness/tightness in my right sacroiliac area. Nothing serious, just a bit stiff. Enough to notice it was out of the normal. It was a little worse on Saturday and on the easy run that I went on, it was causing some bother. Enough to think I’d have a few rest days.
Sunday – I could barely put any weight on my right leg because of the pain in my lower back. It was like a needle being forced through the auricular surfaces of my sacroiliac joint. I had not bashed it, no acute injury, just ache on one day followed by pain the next.
Hmmm.
What to do?
Initially, no panic. Just rest. No point in running on it if it just makes it worse. A week went by- no improvement, and I was hobbling around at work – in more pain than a lot of my patients! The next week I was due out in Chamonix to recce some of the race route. I managed a 20km day on pain killers, but the planned 30km day – what should have been a doddle, was curtailed at 2km because I couldn’t even walk let alone run.
Crap.
7 weeks to go before the race and I can’t even train. I’ve been in similar situations, so no real issues, I’ll just be a bit slower than I’d hope.
2 weeks later still no improvement, despite my attempts at rehabilitation, and eventually I went to see a local osteopath to see what he thought. Classic MSK stuff followed with hip upslips etc, but the “weird” thing was that my right hip was moving “perfectly” but my left hip was “stuck”. Odd… my left hip felt amazing. If only I could have two of those!
So no new information I didn’t already know as a physiotherapist.
Anti-inflammatories weren’t touching it, painkillers didn’t really work, so it was really just a case of getting back to the drawing board. Searching for “SIJ pain” online brought up a heap of outdated and useless treatments that really weren’t working.
The best diagnosis I could offer myself was that I had chronically overtrained and had somehow affected the nerve-endings in my right sacroiliac area and it was going to take quite a while for them to get back to normal. In the meantime, I could strengthen muscles around it and try to keep it as normal as possible in terms of what I do, and if that meant not upsetting it by not running, so be it.
7 weeks later it still wasn’t better, and although walking is ok and painless, running a 110km race was going to be out of the question. To be fair I could have walked it, but that would have rendered me even more injured at the end of it, and probably taking more months away from running afterwards. I took the sensible decision and wrote my withdrawal letter. A DNS is much more preferable to a DNF.
Now
So here I am at the beginning of September a few days after I should have finished my main race for the year. Although I am without SIJ “pain”, I can still feel a little “something” in the area where it started – there is also the ongoing hip flexor/adductor problem. My hips are still anteriorly tilted and any “core strengthening” I attempt to do makes it hurt.
Bringing this back full circle, it really does FEEL like a mismatch between my hip flexors – too strong – and my “core” – too weak, with the resulting problem manifesting itself in the middle, where the two pulling powers meet… funnily enough, directly opposite that, in my back, is the SIJ position that reduced my TDS hopes to nothing.
I am trying to redress the balance, to enable myself to extend my hips – that is my femur, without creating excessive anterior hip tilt and lumbar lordosis. Stretching does not seem to help the range of motion, so strengthening the muscles might do…. But I’m finding that physically pretty challenging to do.
What the people in the know say:
Adam Meakins – research pedant and evidence based practice champion – SIJ laxity is NOT a cause of pain. Also – SIJ stability is NOT a cause of pain. There may be pain due to overload and excessive forces across the joint making nociceptive nerve endings start to complain… the key is looking at irritability, severity and pain provocation patterns and dealing with them. So far so good – and pretty much what I have been following and doing so far.
Greg Lehman – has reservations about the relevance of reduced hip extension to pain and injury – however he is open to the possibility that reduced hip extension in runners can influence function – in terms of creating overstride patterns, increasing metabolic cost and increased impact loading.
Jerry Dicharry suggests that decreased hip extension can compromise efficiency and may increase injury risk… but not SIJ injury specifically.
In terms of “Lower Crossed syndrome” there is precious little science that says reduction in hip extension means you’ll compensate for it by increasing the lumbar lordosis in a kind of regional interdependence – which will end up with an increased chance of injury.
Plans
Now, I know that scans are a bit of an interesting thing, and that by getting one, there might very well be nothing to see apart from a set of hips that are 37 years old. However, as a “patient”, I’m running out of patience with myself and the rehab. If this thing doesn’t get better by the end of September I’m actively considering getting an ultrasound and an MRI. Which to my physio head seems nuts (because physical appearance doesn’t give an indication of why something hurts. Imagine going to a computer repairman and they open your computer to look at the innards, do it back up again and send you on your way. Just LOOKING at the components doesn’t give you an idea of what is going on) … but to my injured self seems like a thoroughly good idea.
I feel certain there is no hernia anteriorly, but that doesn’t seem to be healing – or getting less symptomatic, there appears to be no diagnosis that I can find or think of (apart from maybe inflammation of the pubis) that makes sense. Nor have any of the people I have talked to in various professional situations…. And the whole pain in the SIJ… nothing of any type of sense appears to have been proffered by any theory or syndrome out there.
I have no issue with not running for the moment. I haven’t run properly in 8 weeks, (though have managed a few 5km shuffles) but I still don’t know what is going on here, and neither does anyone else.
As far as I know, the injury has come about because of chronic training on a theoretical Lower Cross Syndrome – but I can’t seem to find a way out.
Am I being impatient? Am I getting things wrong? Is Lower Cross actually a Syndrome that is causing this? (if so, why haven’t I ever had this pain before?).
So many questions, and for an evidence based therapist – a lot of dead ends.
One thing is certain. I am not looking for a magic wand. I am not looking for something that miraculously heals me. I’d love to know what is going on, whether it be biomechanical, or simply neural… and how to get back to running without pain.
The daily rehab and quest for knowledge continues.
If you’re wondering – I will update this in about a month to see where I’m at, and see if anything has touched it in terms of rehab.
Tim